Color perception and diagnostic tests

The color vision
The human retina has two basic types of photoreceptors: cones and rods. Both contain pigments (ionopsin the former, rhodopsin the latter) that make them sensitive to light, but it is the cones that are the photoreceptors predominantly responsible for color vision.
Cones are divided into 3 subtypes, distinguished according to the pigment they contain, which determines their ability to absorb light radiation more or less effectively depending on its different wavelengths (see Figure 1):
- S-type (short) cones, containing cyanopsin, fewer in number than the others (about 7 percent of the total) and absent in the central fovea (the area of the retina with the greatest visual acuity), have an absorption peak around the 430 nm wavelength;
- M-type (medium) cones, containing chloropsin and numerically more numerous, have an absorption peak around 540 nm;
- L-type (long) cones, containing erythropsin, show an absorption peak around 570 nm.
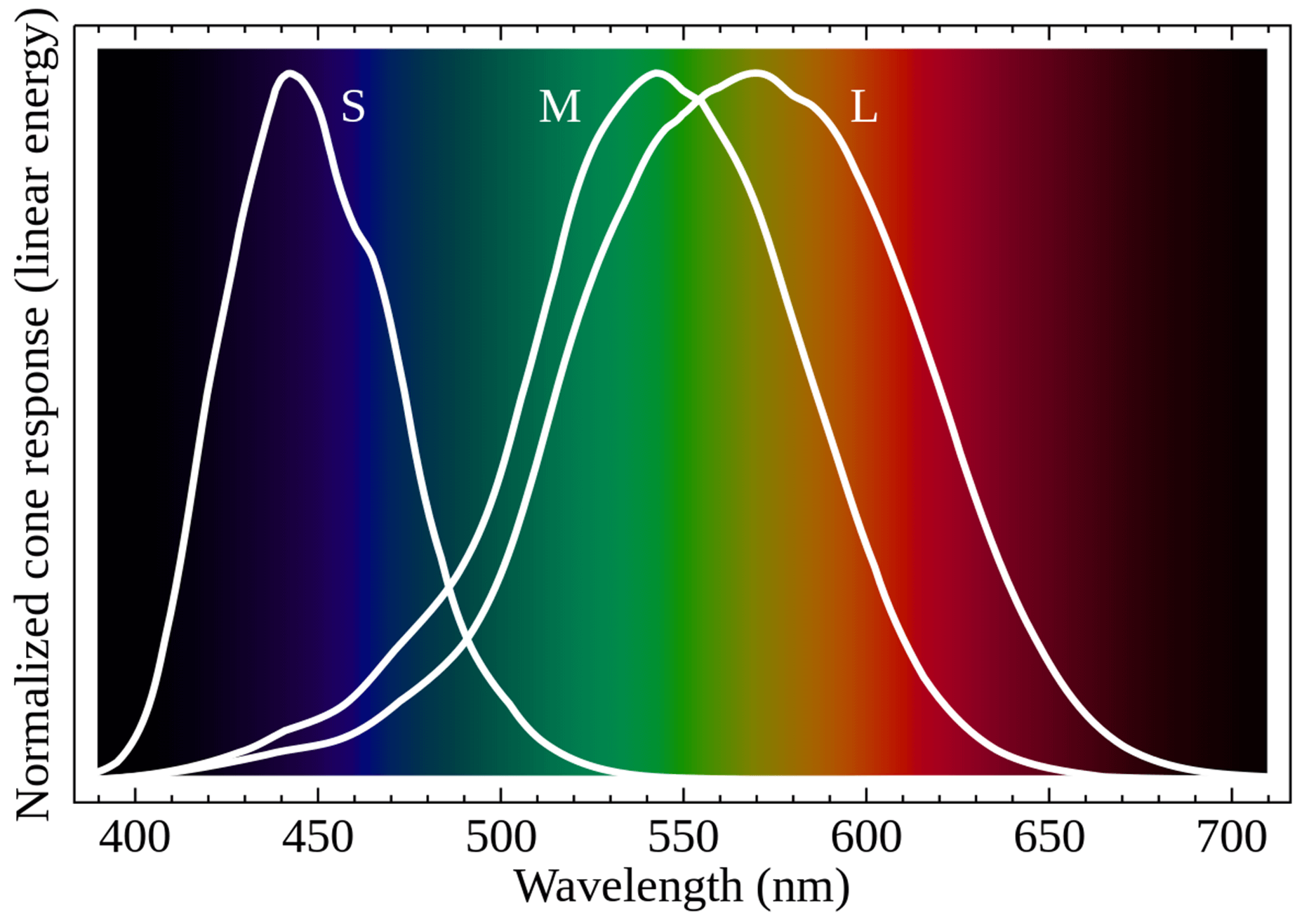
Image taken from Mysore, Aprameya & Velten, Andreas & Eliceiri, Kevin. (2016). Sonification of hyperspectral fluorescence microscopy datasets. F1000Research. 5:2572, licensed under a Creative Commons Attribution 4.0 International license.
Frequently, these three types of cones are referred to as blue cones, green cones and red cones, respectively, referring to the arrangement of these three colors along the color spectrum of light:
- blue is on the shorter wavelengths (S)
- green on the intermediate ones (M)
- red on the longer ones (L).
Although Figura 1 shows how there is no exact correspondence between blue, green and red and the absorption peaks of the pigments contained by the three types of cones, it is very convenient to imagine that just as the combination of a blue, a red and a green light gives rise to a fourth color (different from the three primary colors used), so the colors we perceive are derived from the combined response of the three types of cones.
So we are referred to as trichromatic vision, and humans can normally be called trichromatic.
Within the retina, light information collected by photoreceptors is transmitted via bipolar cells to retinal ganglion cells, combining input from several adjacent photoreceptors.
It is already at this level that color information processing occurs, with cell populations responding oppositely to long and medium stimulation (red-green contrast) and other populations responding oppositely to medium-long and short stimulation (yellow-blue contrast).
The lateral geniculate nucleus then receives via the optic nerve, optic chiasm and optic tract the information, which is kept at least partially segregated:
- information from L- and M-type cones arrives via cells predominantly to the four dorsal parvocellular layers;
- information from the L- and M-type cones is transmitted to the koniocellular layers via the bistratified cells;
- other pathways are mainly responsible for information related to luminance contrast, but not to color.
The signal then reaches the primary visual cortex (V1) in the occipital lobe; here certain areas respond best to specific areas of the light spectrum, although this response is considerably variable depending on the brightness of the stimulus, and cells specifically deputed to detect red-green and yellow-blue type contrast can be identified.
These circuits do not remain entirely parallel, but allow mixing of the red-green and blue-yellow systems to produce responses to magenta (red and blue) or cyan (green and blue), expanding the number of detectable color contrasts. The processing of color information continues in areas V2, V3 and the extended V4 area, combining it with information about the direction and shape of the stimulus, its motion, the language involved in color naming, etc.
Color vision is a complicated psychophysical process: the final sensation concerning the color a subject believes he or she sees is determined not only by the physical stimulation of the retinal photoreceptors by light, but to by the complex processing mechanisms at the retinal and cortical levels, which are also influenced by the subject’s own experience.
For example, some populations whose lives are based on collecting plants have developed special methods of classifying shades of green that enables them to notice and catalog color differences that would be imperceptible to others.
Color vision abnormalities
Humans normally possess three different populations of receptors deputed to the perception of color; in addition to normal interindividual differences, there may be altered functioning at the expense of one or more of these populations that prevents the correct detection of part of the visible spectrum.
If the affected subject maintains trichromatic vision but colors in a given band must be presented with higher than normal light intensity to be adequately perceived, this can be called abnormal trichromatism, distinguished into:
- protanomaly, if the major deficit is found in the perception of long wavelengths;
- deuteranomaly, if the major deficit is found in the perception of medium wavelengths;
- tritanopia, if the major deficit is found in the perception of medium wavelengths.
If an entire population of cones is prevented from functioning, for example because the corresponding pigment is not synthesized, the vision is dichromatic and the corresponding condition can be defined, analogous to the previous cases:
- protanopia;
- deuteranopia;
- tritanopia.
Lastly, if only one class of cones (typically S-type) is functioning we speak of monochromatic vision, with a picture scarcely distinguishable from achromatic vision, in which the only functioning receptors remain the rods.
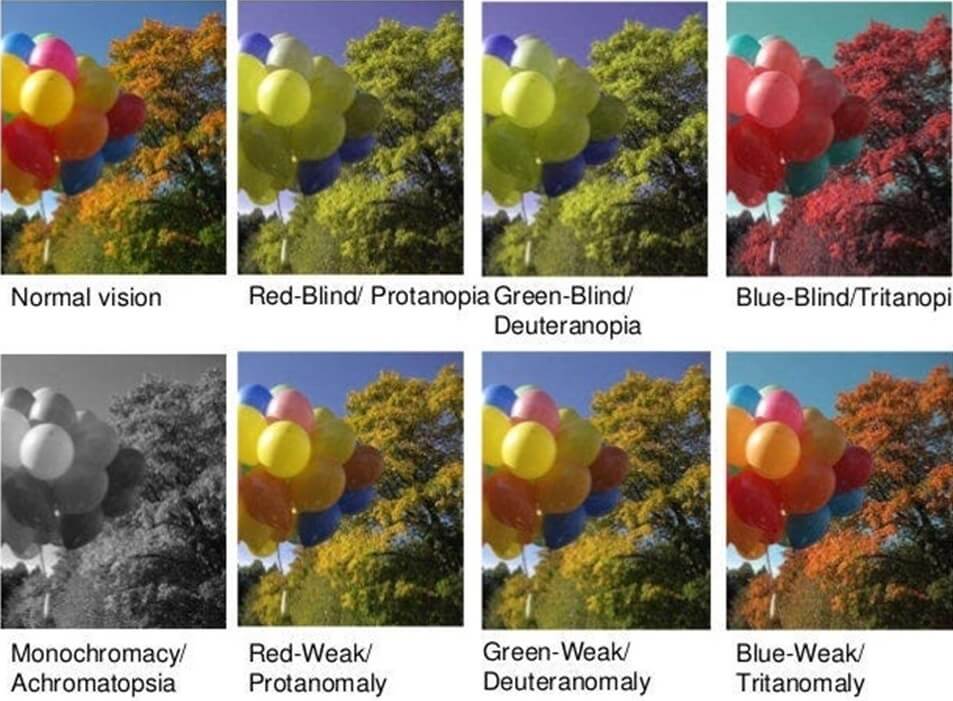
Image taken from the website Coblis – Color Blindness Simulator
The reported classification is especially suited to the description of those genetic conditions that alter or prevent the production of pigments involved in normal cone response.
As mentioned above, the genes coding for the cone pigment for red and green are located on the X chromosome, represented in a single copy in male-gendered individuals who, therefore, manifest the protan- and deuteran-type congenital alterations more frequently than female-gendered individuals.
Abnormal trichromatic vision can have different manifestations depending on how far the absorption curve of the pigment in question deviates from normal, ranging from pictures close to normal trichromatic vision, with no particular consequences, to pictures very close to dichromatic vision.
As for acquired alterations in color perception, these can be found in a wide range of ocular, nervous and systemic diseases, as a consequence of intoxication or even as an outcome of trauma and cancer.
Among the others, Verriest1 categorizes acquired deficits in color perception by analogy with congenital alterations and distinguishing:
- Type I (protanope-like or protanomal), found, for example, in choroidal atrophies, Stargardt’s disease, atropine and ergotamine intoxications;
- Type II (simil deuteranope or deuteranomal), in various optic nerve dysfunction, toxic amblyopia, optic atrophy, peripheral chorioretinal degeneration, myopic choroidal degeneration, rhegmatogenous retinal detachments, central serous retinopathy, and chorioretinitis;
- Type III (tritanope or tritanomal-like), of possible occurrence together with papilledema, glaucoma, multiple sclerosis, methylene blue intoxication and others.
Some cortical lesions can totally prevent color recognition. Another special phenomenon involving color perception is synesthesia, with the appearance of a color sensation triggered by a nonluminous stimulation, such as a sound.
Color sensitivity test
Color sensitivity abnormalities can be assessed by various tests for diagnostic purposes or to evaluate performance in relation to specific job profiles.
Tests can be classified according to the task required of the test subject:
- equalization test, in which a sample color is to be reproduced by an appropriate mixture of light beams;
- discrimination test, in which symbols embedded in mosaics of differently colored dots are to be distinguished;
- naming or comparing, in which colors of colored objects or lights are to be recognized, sometimes by matching them with sample colors;
- classification, in which one must produce correct color sorting of colored objects.
Genetic testing, ocular electrophysiology, and examination of retinal morphology (e.g., by optical computed tomography) may also be useful in specifying the diagnosis and classification of the detected deficit.
Historically and in research, several dozen tests have been proposed for the assessment of color sensitivity. In addition, of the tests commonly used in clinical settings there are several versions with some manufacturer-dependent variations.
The tests that will be presented in the following are only intended to give a nod to some of the existing types of tests.
Pseudoisochromatic tables
There are many tests based on the presentation of pseudoisochromatic tables in print or digital versions, usually detecting mainly congenital alterations in color perception along the red-green axis.
These are tables consisting of colored dots some of which are arranged to form numbers, letters or geometric symbols and others to form a background. The tables are structured to differentiate between subjects who, perceiving colors normally, detect symbols correctly, and those with impaired sensitivity who do not see symbols present or, conversely, see symbols that should be hidden (see, for example, Figure 3).
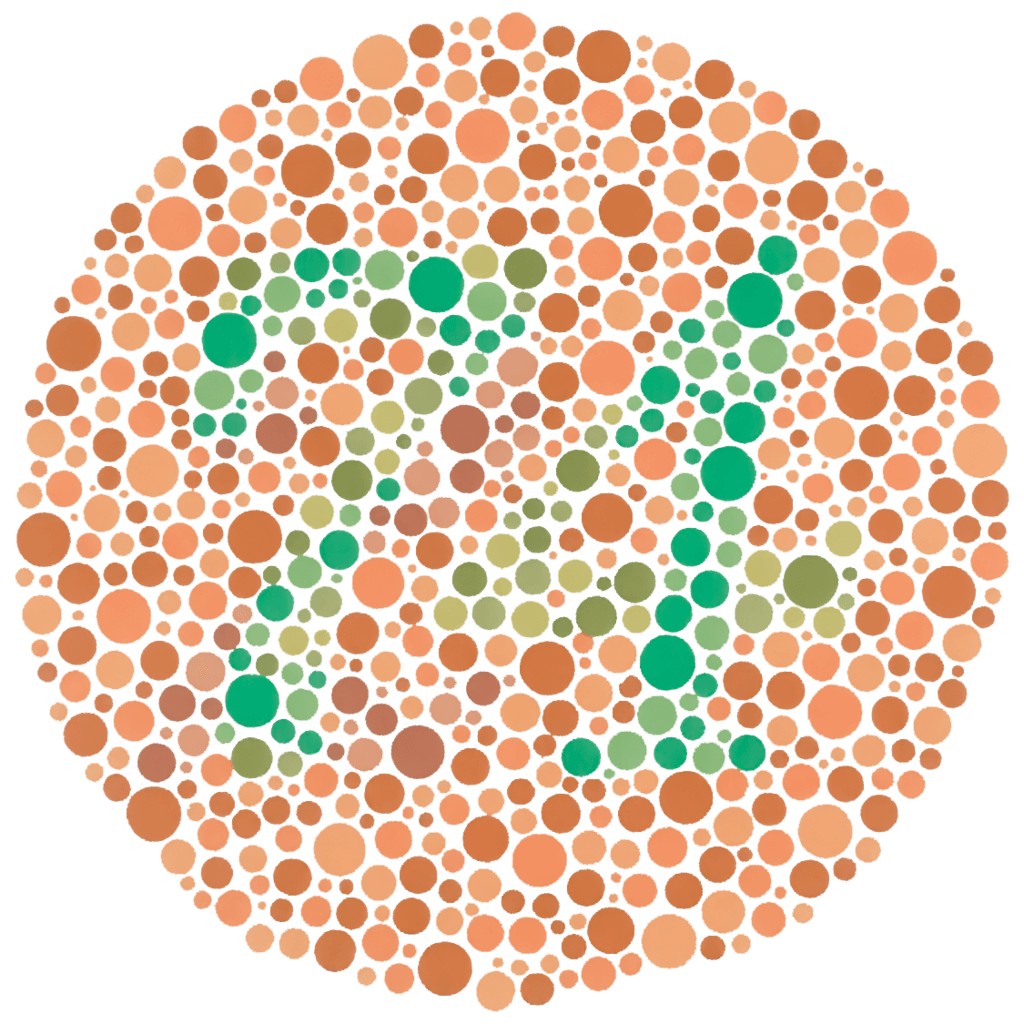
Image taken from the website Color Blindness
Some tests, for example the American Optical Hardy-Rand-Rittler (Figure 4), also assess tritan-type deficits and give an estimate of the level of color sensitivity impairment.
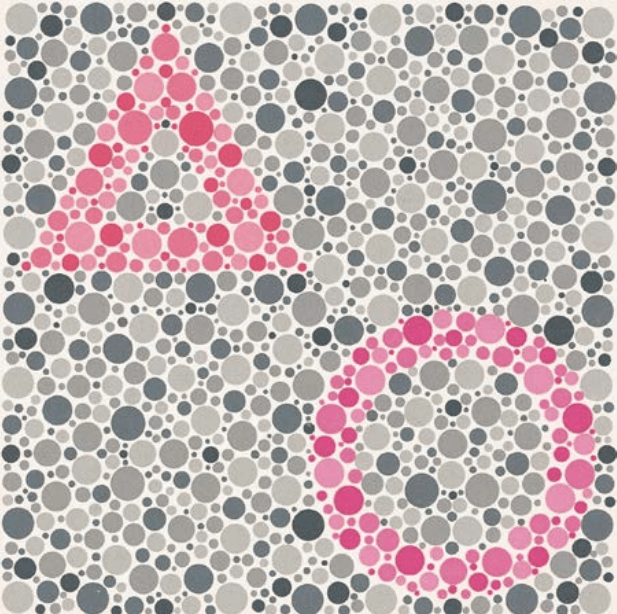
Image taken from Alex Melamud, Stephanie Hagstrom & Elias Traboulsi (2004) Color vision testing, Ophthalmic Genetics, 25:3, 159-187
Anomaloscopes
To give an idea of the operation of anomaloscopes, which are not widely used in clinical settings, we refer here to Nagel’s anomaloscope (model I) and the very similar Neitz OT; other anomaloscopes have similar operation and can be differentiated, for example, by the variety of chromatic reference stimuli (e.g., Pickford-Nicolson anomaloscope).
The observed stimulus consists of a circle whose lower half is yellow (589 nm) and of adjustable brightness and the upper half is colored with a mixture of yellow-green (545 nm) and red (679 nm) light in adjustable proportions. By adjusting the brightness of the lower half of the circle and the color mixture of the upper half, the examinee is asked to compare the two halves. If he or she believes equality has been obtained with values outside the norm and/or equality has not been achieved with normal values, one has abnormal trichromatism or dichomatism. The breadth of the range in which the subject’s chosen color proportions fall and their mean value allow one to direct the diagnosis.
Lantern test
Lantern tests consist of the presentation of lights with the anteposition of different filters for color (typically in the range of greens, whites and reds), brightness and texture, or corresponding stimuli played on a monitor. The subject is asked to correctly identify and recognize the presented stimuli. The purpose of these tests, which exist in various versions, is usually to assess suitability for performing specific tasks in the transportation and armed forces sectors.
Classification tests
Classification tests are, introduced in the 1930s, exist in multiple versions and are widespread in both their traditional, colored-disc versions and their digital versions. Some of the most famous include Farnsworth–Munsell 100 hue test (see Figure 5), the Lanthony New Color Test, Roth’s 28-tone test, Farnswort’s D-15 test, and Lanthony’s desaturated D-15 test.

Image taken from Farnsworth Munsell 100 HUE test
In all cases, the test subject is asked to sort the colored dowels starting with a reference color (sometimes arriving at a second reference color). The type of deficit is determined on the basis of the disposition errors; in particular, when these are polarized along a specific axis, they may allow more specific targeting of the diagnosis (see Figure 6).
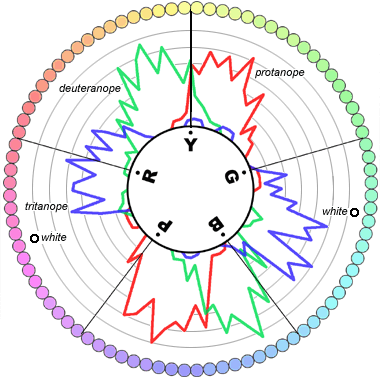
Image taken from Prism – Update Bulletin of the Italian Association of Assistant Orthoptists in Ophthalmology – Year 2008, n. 1, p. 17
Conclusions
Color perception, which greatly enriches in detail what we observe, translates the different wavelengths of which visible light reaches our eyes into different sensations through a complex mechanism that includes the photoreceptors housed in the retina, other retinal cells, visual pathways up to the occipital cortex, and cortical-level processing of color information.
Sometimes this mechanism can function abnormally due to congenital, often genetic, or acquired causes, impairing the ability to distinguish certain colors normally or preventing the detection of certain shades altogether. Through some specific tests it is possible to detect and classify the perceptual deficit, making it possible, for example, to obtain additional elements for the diagnosis of certain pathologies, to better direct the rehabilitation of visually impaired subjects with associated difficulty in color perception, and to assess suitability for performing certain tasks that require excellent color discrimination skills.
Essential Bibliography
- Verriest G. Further studies on acquired deficiency of color discrimination. J Opt Soc Am 1963;53:185–95
- Alex Melamud, Stephanie Hagstrom & Elias Traboulsi (2004) Color vision testing, Ophthalmic Genetics, 25:3, 159-187 –
- Conway BR, Eskew RT Jr, Martin PR, Stockman A. (2018) A tour of contemporary color vision research, Vision Res, 151, 2-6
- Andrew Stockman (2019) Cone fundamentals and CIE standards, Current Opinion in Behavioral Sciences, 30, 87–93
- Stephen J Dain (2004) Clinical colour vision tests, Clin Exp Optom, 87:4-5, 276-293
- Samuel G. Solomon, Peter Lennie (2007) The machinery of colour vision, Nature Reviews Neuroscience, 8, 276-286
- Kaur K, Gurnani B. (2022) Revisiting Color vision standards and testing methods in various occupational groups, Indian J Ophthalmol, 70(1):329-331
Talk to a visual rehabilitation specialist now
Contact us without obligation to receive information.
Our Specialists will respond to you Monday through Friday from 9:00 a.m. to 5:00 p.m. (CET).
You are free to reproduce this article but you must cite: emianopsia.com, title and link.
You may not use the material for commercial purposes or modify the article to create derivative works.
Read the full Creative Commons license terms at this page.
You may also be interested in...

Stuttering: what is it, symptoms, and how to deal with it
Stuttering: what it is, how to distinguish symptoms, and how to improve quality of life.


Squint: types, symptoms and treatments
The causes of this problem are numerous, each of which contributes to describe the characteristic features of the various types of squint.


Attention deficit and hyperactivity: how to recognize it?
Attention deficit and hyperactivity disorder may be due to a multiplicity of factors, among which the most likely are genetic.


Diplopia: what are the causes and cures
Causes, symptoms and treatment of “Double Vision” or Diplopia.
Neurodevelopmental disorders: what do they entail?
Neurodevelopmental disorders make their onset in childhood and may persist into adulthood.

Verbal language in autism: how to communicate?
What are the communication problems involving verbal language in autism? Here’s how to act on this issue.